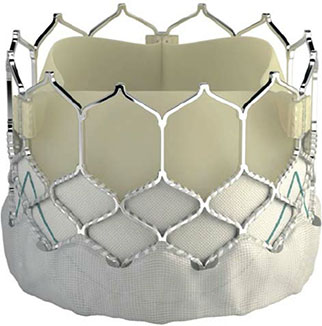
Dr Malik gave a Talk on Transcatheter Aortic Valve intervention (TAVI) to Care of the Elderly Physicians in London.
- What is it
- How do you do it?
- Who is suitable?
- Who is not suitable
Dr Malik says: “The role of TAVI is increasing as the risk of the procedure goes down. It is now possible to quote a 1% mortality in many centres. However, if you are very sick, TAVI can be life saving. I gave this talk to Care of the Elderly Physicians in London. It was an honour to be invited to speak. It gives a summary of ‘How, Why and Why Not’ for TAVI procedures. Have a look!”
Watch it here!