If you have a heart attack, you are often best managed by going direct to a Heart Atack Centre (HAC), where you are immediately assessed to see if an emergency operation to open the blocked blood vessel (a Primary Angioplasty and Stent) is suitable. In the whole of London, these HACs provide 24/7 coverage, 365 days a year.
What about Stroke?
Unfortunately, if you ahve a stroke, even if you get taken to a Hyperacute Stroke Unit (HASU), you may not be offered the same treatment as for the heart. Why? Several reasons:
No 24/7 rota for Mechanical Thrombectomy (MT) or clot extraction- not enough skilled operators
Too late to benefit
wrong type of stroke
Dr Malik and his team have publised a review of the evidence base- we have had many trials looking to see if MT works. It does, and saves lives. Logistic and political issues prevent it being delivered. Dr Malik works at Imperial College Healthcare NHS Trut where it is now delivered to those who need it 24/7, 365 days a year. It is hoped that other centres will follow soon!
Cholesterol is a risk factor for heart attack and stroke
Multiple trials show the link between high cholestrol and cardiovascular disease. The great news is that it is modifiable- just like smoking, high blood pressue and even diabetes. The non modifiable ones are your age (you can’t get younger), your gender, your race (south asians are at elevated risk) and your family history (you can’t change who your family are!)
Reducing Cholesterol lowers risk
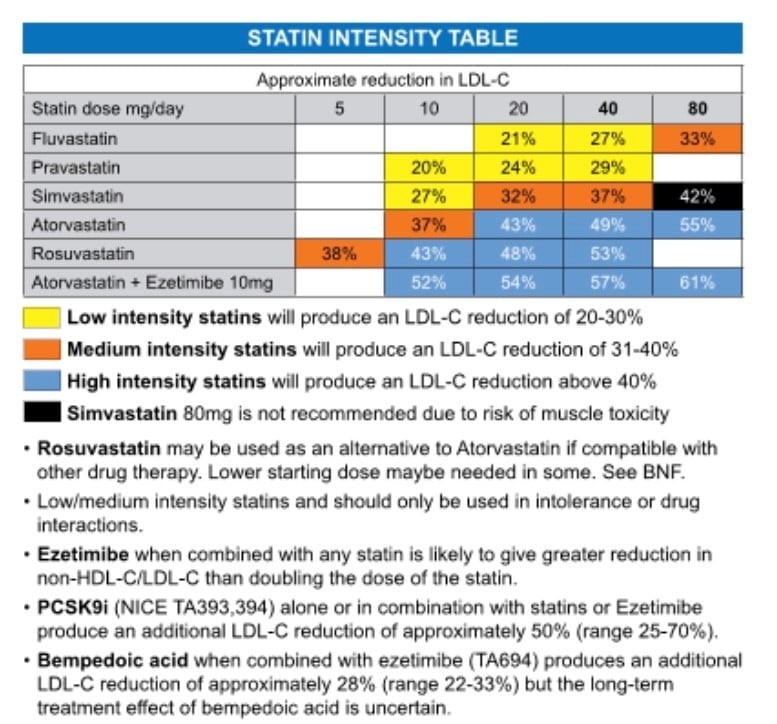
You can lower choleterol by about 10% with diet and exercise. Statins lower it by about 30%. Different statins have variable effects. And adding Ezetimibe seems to help more than doubling the statin dose, perhaps with fewer side effects.
How low should I go?
In my mind, the lower the better- If you have had a heart attack I would like the LDL <1.4 mmol/l.
Dr Malik read a news story with interest: “Fasting regenerates the pancreas in Diabetes Mellitus (DM)”
However, this was a study in mice that were genetically prone to DM. They had 4 days severe dieting (perhaps an equivalent of 1000 calories, but mainly as fat, not carbohydrate or protein), and then a normal diet for 3 days. This was repeated.
Beta-cells in the pancreas make insulin. It seems that periodic starvation could get their beta-cells (which were withered away), to reactivate or regenerate. In non diabetic mice, they found a drop in beta-cells activity in the diet, which could of course be alarming, but a recovery within 24-48 hours, and a better gene activation pattern. So the beta cells could be “tuned-up”.
Weight Loss is good for you
Weight loss is known to be important in treating type 2 DM in humans. Calorie control is vital in prevention and treatment. Bariatric surgery is now also a validated treatment for severe diabetes. So is pancreas transplantation. This study suggests that you might be able to “auto-transplant” a better pancreas into yourself by dieting.
DONT try this diet at home without medical advice. High fat diets also have risks. Losing weight gradually is a good idea. Long periods of starvation (as in famines and world wars) have been known to increase the lifespan of survivors, but how to apply that in daily life in the world today has not been fully worked out.
Mouse research can take a decade to get to a human equivalent.
I often tell patients with palpitations and even blackouts that coffee and tea may be the cause. Stopping it may avoid more investigations and invasive treatments.
Where did coffee come from?
This site takes you through the origins of coffee. It appears that dancing goats in Ethiopia lead the goat gerder to look for the cause- coffee beans that they had eaten. Now it is one of the largest commodities traded in the world. And it tastes good!
Although originating in the Muslim world, initially declared “Haraam” or sinful, and then declared “Hala” or permissible by the Ottomans, Pope Clement VIII sampled coffee for himself and decreed that it was indeed a Christian as well as a Muslim drink.
Inside the red fruit of coffea lie two green coffee “beans”. The rich brown hue to appear only after roasting. In fact, they are fruit, and the seed is the coffee bean you need!
Evidence of benefit
Here is a tale from a very worthy journal suggesting that high coffee intake may be linked to reduced mortality. It was a randomised trial. This is the gold standard of evidence. BUT still it is by no means certain that these high coffee drinkers were not different from the non coffee drinkers in some other way, although the study did try to control for smoking habits, social class, body mass index etc.
Downside?
It will make you pass water. It can give you palpitations. It can make you anxious and irritable. It might increase your heartburn. And the Buzz can wear off. Evidence suggests there can be a reliance on the drink, and tolerance builds over time.
Finally, it can be addictive. So beware. Going cold turkey now and again will keep the addictive tendancies at bay. Withdrawal symptoms include a headache, fatigue, irritability, difficulty concentrating, and depressed mood.
Message
If you like coffee and are not getting side effects, then keep on going. There seems no need to cut back on this ubiquitous and legal “high”.
Professor Sir Bruce Keogh, previously Medical Director of the NHS, and a cardiac surgeon by trade, said all surgeons should have their operation statistics published. He felt that doing so would make the surgeon more careful. The risk taken would not be just for the patient, but would now also hang over the surgeon.
This seems obviously a great idea.
But hang on a minute…
Like all issue, it is more complicated than it seems.
Did it mean that some surgeons were previously “gung-ho”- I have not come across those- most are very balanced on their approach to risk.
Will it mean surgeons will practice more safely- perhaps- if they were “gung-ho” in the 1st place, but perhaps it will make them risk averse. That is, they will refuse to take on the higher risk cases-as that will reflect badly on their Stats. This is the same as the school not entering your child in for an exam because they wont get a grade 7,8 or 9, and that will reflect badly on their school performance table.
So, the outcomes have to be risk-adjusted
If the expected death rate is 5% from the surgery and the surgeons ouctome are 5%, then she/he is performing as expected.
If in fact their outcomes are 3%, they are better than expected (or the risk scoring system is out of date- as all surgery is improving as time goes by- remember a Victorian era surgeon would chop a leg off without anaesthetic or antibiotic!).
If they are performing worse- say 7% death rate:
it could be that the risk scoring system is not taking some other factor into accout that is vitally important (eg frailty of the patient- which is easy to judge in front of you when seeing the patient walk in, but hard to quantify).
Or the surgeon as not done as many cases to even things up, and a play of chance has made the stats look bad.
Or of course, there is a genuine problem that needs to be looked into- This is rare
So. Do you want a surgeon with very low mortality for their procedures- YES
But. Do you want a surgeon used to dealing with high risk cases-YES because they will find the easier cases very simple and get great results. BUT this surgeon will a mortality rate that will of course be higher than for the average surgeon.
Conclusion
It is hard to know who is “the best”. A personal recommendation by someone in the know is probably better than searching for statistics that are harder to interpret. On average surgeons, including interventionalists like me, get appointed as Consultants (in USA speak, “Attending Physicians”) at about 35-40, and reach their peak of experience 45-55- when they have been around long enough to know all of the issues, experienced all of the complications, and thus know how to deal with them. Their data is also more stable- as they have done so many cases that their average mortality is a true representation of what they do.
UK surgeons are now moving AWAY from individual surgeon data, but presenting data for their unit. If the whole unit data is looking bad, then individual surgeons data should be examined. This makes more sense to me.