At the Abbott Heart Symposium on TAVI, you had the chance to try a Virtual Reality headset.
This amazing tool lets you walk in and out of a heart and explore it from all angles!
With the headset on, I could see nothing but the heart and moved around using the two-hand controllers. An expert guided us, “slicing” the heart to show key features such as the aortic valve, mitral valve, and left atrial appendage.
This 3D view of the heart is great for beginners to understand its structure.
I can see how we might use this to plan complex congenital heart disease procedures. For example, by inserting differently shaped equipment into the virtual model. Currently, we do this by 3D printing a model and physically inserting the devices.
This VR system could become even more useful in the future, helping us plan heart procedures more effectively.
Article by Dr Malik, a UK leading cardiologist. He works at One Welbeck Heart Health – London’s Largest Private Cardiology Group, and at Hammersmith Hospital, Imperial College Healthcare NHS Trust, London, one of the largest NHS Trusts in the UK.
I had the pleasure of being on the faculty for this year’s Abbott UK and Ireland annual meeting. Just like last year, I was enthusiastic about the opportunity. I chaired the midday session, engaging a diverse audience of consultants, trainees, and healthcare professionals, encouraging them to think and participate actively.
Sponsored by Abbott, the meeting naturally focused on their TAVI valves. The latest version, previously known as Portico and then Navitor, is now called Vision.
What Did I Learn?
We were introduced to some fascinating 3D virtual reality aids designed for teaching doctors anatomy, allowing them to “walk through” the heart. While it’s not yet useful for planning complex TAVI procedures, I believe it will be in the future!
Having a surgeon present was beneficial as well. We debated how young a patient can be to undergo a TAVI. My youngest patient was 30, with complex heart disease and two previous operations. We performed an emergency TAVI with great success, which will lower the risk for future surgeries, sorted the acute leaky valve, and gave the heart time to recover.
In the USA, people in their 60s often demand and receive TAVI procedures. However, the fastest-growing surgical procedure there is removing failed TAVI valves. Hence, every patient I perform TAVI on goes through a thorough discussion process, including a Multidisciplinary Team Meeting (MDT). This ensures that the safest and best option is chosen for both the present and the next 20 years, whether it’s TAVI, surgery, or simply watching and waiting.
Additionally, we discussed precise valve sizing for each patient. This involves accurate CT scan measurements, assessment of coronary anatomy, calcium distribution, other heart diseases, the risk of needing a pacemaker, and, especially for younger patients, planning for the next procedure in 5-10 years.
What Is New?
Abbott has launched the Vision valve with markers for perfect deployment. It’s a self-expanding valve, and we saw it in action during the meeting.
Medtronic introduced the Evolut FX Plus, which is more flexible and has larger gaps to facilitate future coronary artery access. This is also a self-expanding valve.
Edwards presented the S3 Ultra Resilia, featuring a new anti-aging treatment. It’s a balloon-expandable valve.
Summary
I always choose the right valve for each patient, having used products from three different companies so far, with more innovations on the horizon. It’s always a pleasure to be invited to such meetings, especially to chair interesting and educational sessions. Every good teacher knows that every day is a learning opportunity.
If you have any questions about the procedure, don’t hesitate to contact us today.
Article by Dr Malik, a UK leading cardiologist. He works at One Welbeck Heart Health – London’s Largest Private Cardiology Group, and at Hammersmith Hospital, Imperial College Healthcare NHS Trust, London, one of the largest NHS Trusts in the UK.
Dr. Malik is excited to share a significant milestone: the first NHS Transcatheter Aortic Valve Implantation (TAVI) using the Edwards S3 Ultra Resilia valve at Hammersmith Hospital.
In this video, you’ll meet Dr. Foote, an 82-year-old retired doctor with severe symptomatic aortic stenosis, who graciously allowed us to film her procedure. Here’s what the video covers:
Choosing the Correct Treatment: Surgery (AVR) vs. TAVI Valve Selection: Size and Type TAVI Procedure: Step-by-Step Demonstration
The case took exactly one hour, and the video is 16 minutes long. It’s an excellent resource for doctors learning about TAVI, and patients and their families who want to understand the procedure.
I am incredibly grateful to Dr. Foote for her willingness to be filmed and my dedicated team at Hammersmith Hospital, where we perform over 350 NHS TAVI procedures annually. This programme continues to grow, and TAVI remains a life-changing procedure.
Special thanks to Edwards Life Sciences for providing early access to the new Resilia TAVI valve before its official NHS launch.
If you have any questions about the procedure, don’t hesitate to contact us today.
Article by Dr Malik, a UK leading cardiologist. He works at One Welbeck Heart Health – London’s Largest Private Cardiology Group, and at Hammersmith Hospital, Imperial College Healthcare NHS Trust, London, one of the largest NHS Trusts in the UK.
I recently attended my favourite meeting of the year, CSI Frankfurt, which covers all aspects of structural heart disease, from birth to 100 years old! This year, I had the opportunity to discuss topics such as PFO, ASD, and TAVI.
Before arriving in Frankfurt, I broadcasted a live case from my NHS base at Hammersmith Hospital, showcasing a challenging paravalvular leak. The procedure was a great success, and I’m excited to share the video and notes from the meeting once I wrap up my talks.
Article by Dr Malik, a UK leading cardiologist. He works at One Welbeck Heart Health – London’s Largest Private Cardiology Group, and at Hammersmith Hospital, Imperial College Healthcare NHS Trust, London, one of the largest NHS Trusts in the UK.
Dr. Malik has been at the forefront of developing heart attack treatment in the city for over 15 years.
Why has he dedicated his career to this?
He was a founder member of The Pan-London Heart Attack Group, which has significantly improved care for heart attack patients across London. Dr. Malik represents the Heart Attack Centre (HAC) at Hammersmith Hospital, where he is an NHS consultant. The HAC team meets regularly to discuss ways to reach even better results.
Dr. Malik recalls his early days as a trainee at Hammersmith Hospital. He witnessed it become the first 24/7 HAC in London, providing round-the-clock care for patients brought directly by the London Ambulance Service (LAS). Royal Free, Bart’s, St George’s, Harefield, St Thomas’s, Kings, and Hammersmith all work in conjunction with the LAS.
“I still wake up at night to respond to emergency calls and open blocked blood vessels. It’s so rewarding to see patients recover immediately. Luckily the ambulances have become more high-tech these days, but I liked the look of this old bus!” – Dr. Malik.
Article by Dr Malik, a UK leading cardiologist. He works at One Welbeck Heart Health – London’s Largest Private Cardiology Group, and at Hammersmith Hospital, Imperial College Healthcare NHS Trust, London, one of the largest NHS Trusts in the UK.
Transcatheter aortic valve intervention (TAVI) treats severe aortic stenosis with a minimally invasive procedure. Over the age of 75, it is not becoming the treatment of choice over conventional heart surgery.
You need careful assessment to decide
1. If you need treatment
2. How that treatment is done
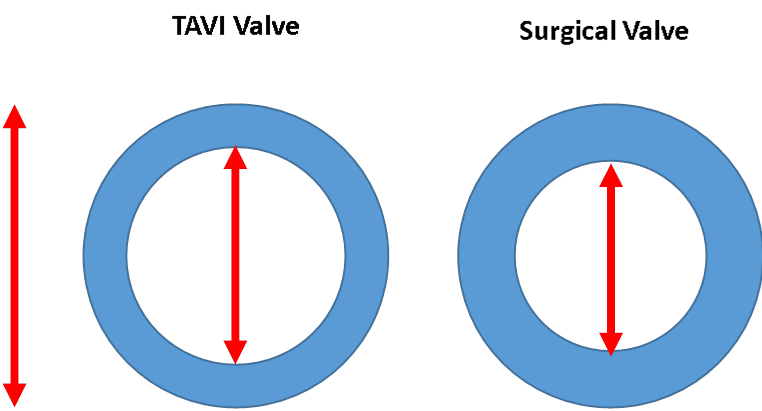
Figure 1: Internal versus external dimensions
Who are Edwards Life Sciences?
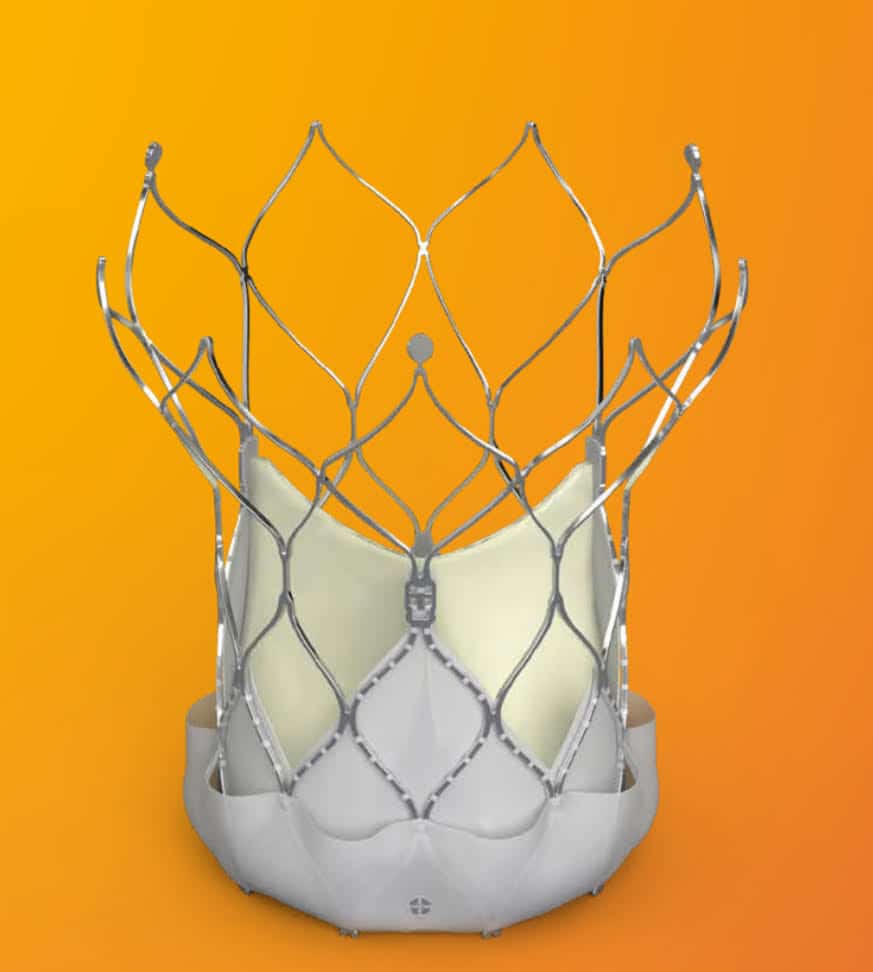
The Edwards TAVI valve is a phenomenal technology, that uses cow heart lining (Bovine pericardium) to hand make a new aortic valve, inside a metal frame.
Thus can be squashed to make it fit into a small pipe to get form the groin to the heart.
Figure 2: The Edwards S3 Ultra Resilia TAVI valve
What is a Proctor?
When other doctors are learning how to do a procedure, or have a challenging procedure where they have less experience, they can “ phone a friend”.
More formally, a Proctor can be asked to help.
By definition, a Proctor is a senior clinician, with a lot of experience in teaching and performing the procedure.
Having been a senior clinician for many years, not only have I trained doctors in my own hospital, I am a proctor for many procedures outside of my hospital, including PFO closure, ASD closure, Paravalvar leak closure, and TAVI.
Every day is a school day
I constantly learn, and this meeting was no exception.
1. Why can the Edwards valve not be squashed even smaller than the 14 French (about 5-6mm) that it isnow.a. Because the collagen fibres in the cow tissue will probably be broken. And although the valve would look the same, it would not last.
2. Why cow tissue, and not horse, pig, kangaroo or some other animal?
a. Cow tissue seems to have better strength, is a bit thicker, and thus may last longer. Pig tissue is thinner, and so could be squashed more, but is more prone to tearing.
b. Edwards now have advanced tissue treatment to try to reduce calcium deposits on the valve– the main mechanism for the tissue getting stiff, and thus the TAVI valve failing. This Resilia technology is fascinating (figure 2)
3. How do we assess any residual narrowing across the new valve.
Figure 3: CT versus echo versus Invasive hemodynamics
a. It won’t be as good as the valve you are born with
b. TAVI seems to be better than a surgical valve of the same size; the external size is whatis stated, and the internal size depends on the thickness of the structural material- which is thinner for TAVI than for surgical valves
c. Assessment with anatomy (really that is with CT scanning), assessment with echocardiography (using pressure gradients) and invasive pressure monitoring (at the time of TAVI) are all slightly different in the way they assess “how good” the new valve is. (Figure 3)
d. Patient –Prosthesis Mismatch (PPM) is hard to assess.
e. A residual “gradient” on echo does not necessarily mean e need top intervene- especially if there are no symptoms.
f. Flow and heart rate function are a bigdeterminant of gradients- if the heart is weak, the gradients are low- that may not be good.If the heart is strong, the gradients may be a bit higher- more push through the same hole– that may not be bad.
4. How about if we need to do Valve in Valve TAVI?
a. Some great cases were shown, in particular on how to protect access to the coronary arteries as material is put in the way of catheters with surgical and TAVI valves
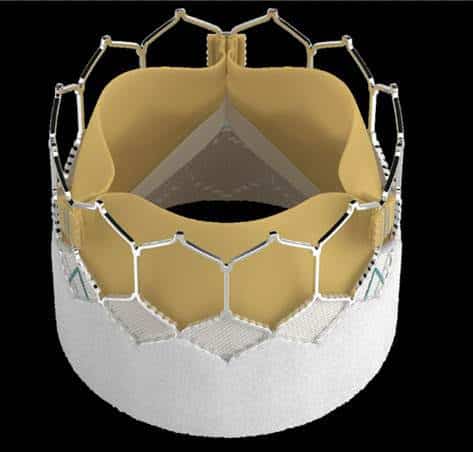
5. How about TAVI in TAVi?
Figure 4: Putting and Edwrads TAVI inside an old TAVI
a. TAVi is so successful now, that it is likely that people who had TAVI 5-10years ago will still be alive, and the tissue in the TAVI valve will now be degenerating, and a further intervention will be needed
b. This marks a real win for TAVI, and these patients were NOT candidates for surgery back then
c. TAVI in TAVI raises its ownissues, and has to be planned even more carefully than Valve in valve TAVI or TAVI in a native (your own) aortic valve. (figure 4). We need to know how to get to the coronaries, see if the old valve leaflets need to be covered or not andto see if we will block the coronary arteries completely- causing a heart attack.
Summary
It was great to share ideas with leading cardiologists and most importantly the engineers who were at the meeting.
I hope they will also take on board my use of invasive hemodymamic assessment in ALL TAVI cases, and the use of guidecatheter extensions when protecting the coronary arteries, ho hep deliver stents and imaging equipment.
Article by Dr Malik, a UK leading cardiologist. He works at One Welbeck Heart Health – London’s Largest Private Cardiology Group, and at Hammersmith Hospital, Imperial College Healthcare NHS Trust, London, one of the largest NHS Trusts in the UK.